Alleviation: An International Journal of Nutrition, Gender & Social Development, ISSN 2348-9340 Volume 1, Number 1 (2014), pp. 1 - 8
© Arya PG College, Panipat & Business Press India Publication, Delhi
www.aryapgcollege.com
Increasing Predilection for Fast Food in Overweight Adolescent Boys of District Kurukshetra
Introduction
Obesity is considered to be a global epidemic, has spread its major roots in both children and adolescents (Lobstein et al 2004). The most important consequence of being obese as an adolescent is its persistence into adulthood with all its health risks. The health risks include hypertension, respiratory disease, several orthopedic disorders, type 2 diabetes mellitus and cardiovascular disease (Must and Strauss 1999). Sedentary lifestyle, unhealthy dietary habits, binge eating, and prolonged TV viewing have probably given rise to this health catastrophe (Gupta and Ahmed 1990, Kapil et al 2002). Metamorphosis of food habits has led to the replacement of nutritious food by things that are tasty, convenient, in vogue-junk food. Food high in salt, sugar, fat or calories and low nutrient content is called junk food. Junk foods provide sub-optimal nutrition with excessive fat, sugar, or sodium per kcal (Anderson and Patterson 2005).
Children and adolescents tend to consume low quantities of fruits and vegetables and have a high intake of fast foods and carbonated drinks (Anderson and Patterson 2005, Neumark et al 2006). Singh and Singh (2008) reported high consumption of fast foods like maggi noodles, burgers, pao-bhaji, sandwiches, hot dogs, patties, pastries, popcorn, potato chips, carbonated drinks, biscuits, muffins, toast, kulcha- channa, samosa, chocolates etc. among adolescents. Adolescent’s eating behaviors are strongly influenced by their social environments, which include family, peer networks, schools, advertising, religion and knowledge (Gomathy and John 2008). Ill effects of regular intake of junk foods are mainly lack of energy, poor concentration and obesity leading to inferiority complex, depression, heart diseases, high cholesterol, stunted growth, premature ageing, and tooth decay (Chhibber 2010). According to a study on adolescents, with excessive consumption of processed foods and high fat diets obesity is on the rise (Augustine and Poojara 2003).
Dietary quality declines from childhood to adolescence, with dietary habits likely to promote fatness being actively adopted (Lytle et al 2000). For example, the consumption of fruits, vegetables, and milk decreases from childhood to adolescence (Lytle et al 2000, Australian Bureau of Statistics 1995), while soft-drink consumption increases (Australian Bureau of Statistics 1995, Lytle et al 2000, & Nielsen and Popkin 2004). Due to increasing allurement of adolescents towards junk food and increasing prevalence of overweight/obesity among adolescents, the present study was conducted to examine and understand the eating behavior of school going overweight adolescent boys in district Kurukshetra, Haryana
Materials and Methods
Selection of Subjects
A sample of 106 overweight adolescent boys aged between 17-18 years was selected by purposive sampling method from two private schools attended by middle and high middle income group students in district Kurukshetra, Haryana
Data Collection
The age of adolescent boys was ascertained by questioning them and later confirmed from school registers. In case of any discrepancy between the two, the date in the school register was taken as accurate. Age in completed years was taken for analysis. A pre-tested and pre-designed performa was used to collect the information on socio-demographic characteristics like age, family type, monthly family income, dietary history and consumption of fast food.
Anthropometric Measurements
Height and weight were measured by using the methods of Indian Council of medical Research (Brahmam et al 2005). Weight was measured using an electronic balance 11
(ATCO) with 100 grams of accuracy. The weight was recorded in kilograms, to the nearest 100 grams. The body mass index (BMI) was calculated as the weight in kilogram/height in meter2 and it was classified according to the classification given by American National Institutes of Health and Heart, Lung and Blood (National Institute of Health 1998).
Adolescent boys having body mass index (BMI) below 18.5 kg/m2 were labeled underweight and between 18.50-24.99 kg/m2 were considered normal whereas, study subjects having BMI between 25-29.99 kg/m2 were classified as overweight.
Statistical Analysis
Data were compiled, analyzed and presented in proportions and percentages. Pearson correlation was employed to determine bivariate relationship. Statistical analysis was undertaken using the Statistical Package for Social Sciences (SPSS) version 16.0
Results and Discussion
General Profile
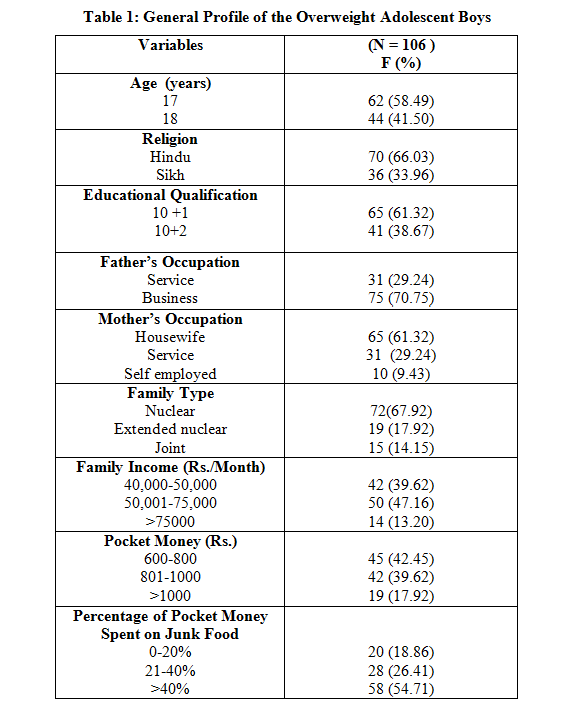
The general information of overweight adolescent boys is shown in Table 1. Out of 106 adolescent boys, most of the respondents (58.49%) were in the age group of 17 years and rests (41.50%) were 18 years old. The subjects were predominantly Hindu (66.03%) and 33.96 per cent of the subjects had faith in Sikhism. Among all the subjects, maximum (61.32%) were studying in XI standard. It was observed that majority of fathers (70.75%) and mothers (61.32%) were businessmen and housewives respectively. Among adolescent subjects, 67.92 per cent had nuclear family pattern, followed by extended (17.92%) and joint (14.15%) per cent. Maximum (47.16%) subjects had monthly family income in the range of Rs. 50,000 - 75,000 and minimum (13.20%) had family income above Rs. 75,000 per month. There were 42.45 per cent of the subjects who received monthly pocket money in the range of Rs. 600 – 800 followed by Rs. 801 - 1000 (39.62 %) and more than Rs. 1000 (17.92%). More than one half (54.71%) of the respondents spent above 40 per cent of their pocket money on fast foods.
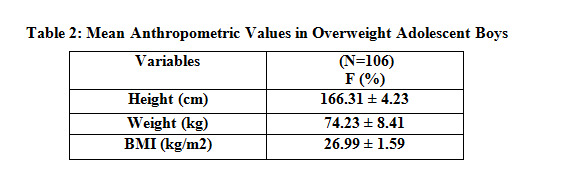
The mean height and weight of the subjects were 166.31 + 4.23 cm and 74.23 + 8.41kg, respectively (Table 2). Body Mass Index (BMI) was used for assessing nutritional status.
The mean BMI of adolescent boys was 26.99 + 1.59 kg/m2.
Dietary Habits
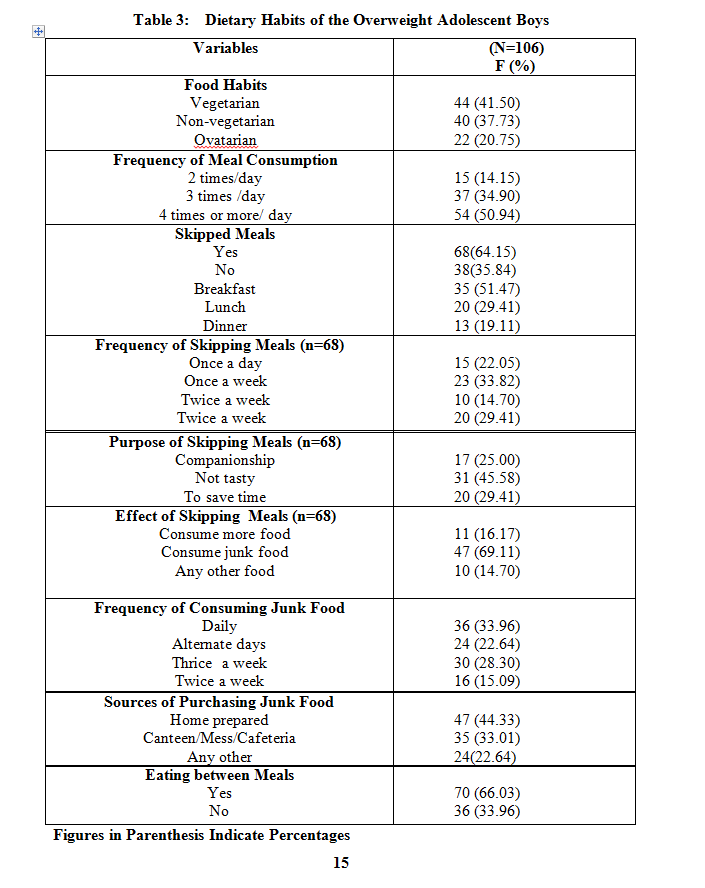
Most of the adolescent boys were vegetarian (41.50%) and pattern of meals consumption per day indicated that one half of the respondents (50.94%) used to consume four or more meals per day (Table 3). Skipping of meals was common in approximately one third of the subjects (64.15%). Commonly skipped meal was breakfast, lunch and dinner among 51.47 per cent, 29.41 per cent and 19.11 per cent of the subjects, respectively. Musaiger and Gregory 1992 reported that skipping breakfast and consumption of calorie-dense foods was quite common amongst Bahraini adolescents. Niemeier et al 2006 found positive correlation between increased fast food consumption, skipped breakfasts and increased body mass index. More than one fifth (22.05%) of the subjects were skipping the meal daily. The main factor responsible for skipping the meals was that it was not tasty (45.58%). Companionship (25%) and to save time (29.41%) were amongst the other factors responsible for skipping the meal. Eating in between meals was one of the causes of unwanted obesity (Jackson et al 2004). Consumption of junk foods was observed among majority (69.11%) of the subjects as a replacement for meal skipping. One third of the adolescent boys were in the habit of consuming fast food daily where as 22.64 per cent of adolescent boys consumed fast food on alternate days. Further, 28.30 per cent and 15.09 per cent consumed junk foods thrice and twice a week respectively. Most (44.33%) of the subjects consumed home prepared snacks while 33.01 per cent and 22.64 per cent of the subjects procured snacks and junk foods from canteens and others respectively.
Junk Food and Snack Consumption Pattern
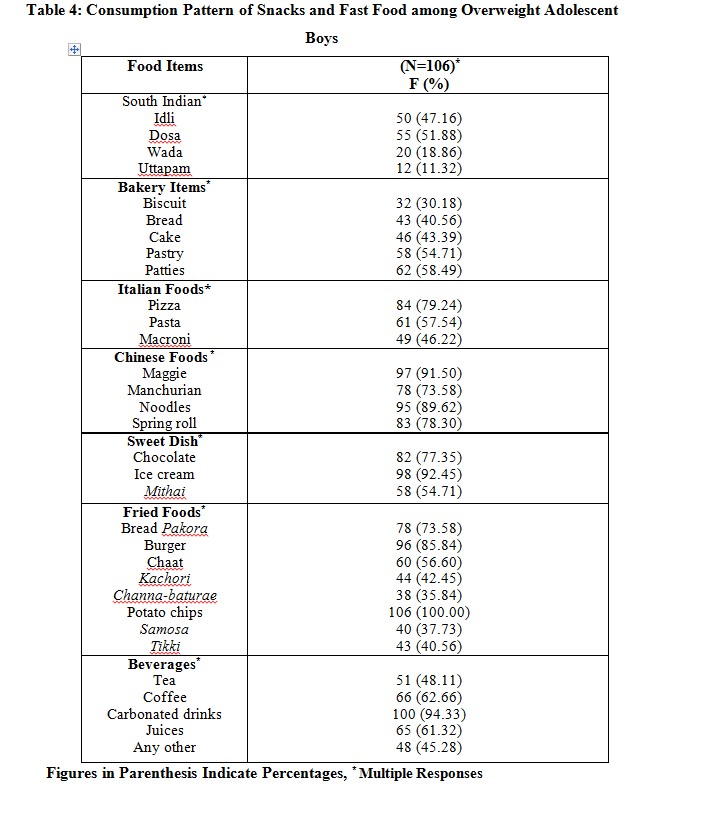
Consumption of various fast foods and snacks among adolescent boys is given in Table 4. Potato chips were the most (100%) preferred junk food item while Uttapam came out to be the least (11.32%) preferred item. It is depicted in the table that 51.88 per cent, 47.16 per cent, 18.16 per cent and 11.32 per cent of subjects used to consume south Indian foods like dosa, idli, wada and uttapam, respectively. Among bakery items, patties were the most favorite (58.49%) snack followed by pastry (54.71%) and cake (43.39%). Bread and biscuits were the least liked bakery items by the 40.56 per cent and 30.18 per cent of the subjects respectively. The most liked Italian food was pizza (79.24%), followed by pasta (57.54%) and macroni (46.22%). Maggie noodles was the most (91.50%) preferred Chinese food item by the subjects. Ninety per cent of the subjects used to consume noodles in routine (89.62%), followed by spring rolls (78.32%) and manchurian (73.58%). Ice cream was the most (92.45%) liked sweet item as compared to chocolate (77.32%) and mithai (54.71%) among adolescent boys. Among fried food items potato chips, burger, bread pakora, chat, kachori, tikki, and samosa were preferred by 100 per cent, 85.84 per cent, 73.58 per cent, 56.60 per cent, 42.45 per cent, 40.56 per cent and 37.73 per cent respectively. Channa baturae was the least liked item (35.84%) among fried food items. These results were consistent with other studies which suggest that junk foods (Bakery items, pizza, burger, cheese, butter, oily items), and chocolate intake tend to be more common among overweight and obese adolescents than among normal-weight adolescents (Klesges 1995 & Wolfe et al 1994). Maximum (94.35%) subjects used to consume carbonated drinks. Coffee (62.66%) was preferred over tea (48.11%) by the subjects whereas, 61.32 per cent and 45.28 per cent subjects liked juices and any other drink (Shikanjee, lemon water etc.) respectively (French et al 2001). Fast food consumption is positively associated with energy intake and soft drink consumption and negatively associated with fruit, vegetable and milk intakes in adolescents.
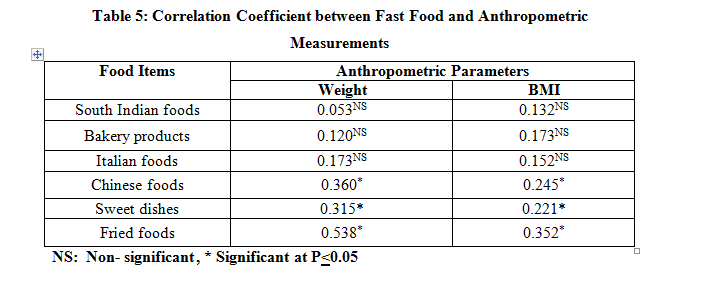
Correlation Coefficient between Junk Food and Anthropometric Measurements:
It is revealed in Table 5 that correlation coefficients were significant (P<0.05) and positive between fried foods and weight and BMI (r = 0.538, r = 0.352 respectively). Significant (P<0.05) and positive correlations were also observed for Chinese foods vs weight and BMI (r = 0.36, r = 0.24), whereas, bakery products and Italian foods showed positive but non- significant correlation with weight and BMI respectively. The consumption pattern of adolescent boys further revealed a positive but non -significant association between south Indian foods vs weight and BMI (r = 0.05, r = 0.13). Ensuing of data further revealed that significant (P<0.05) and positive correlation among sweet dishes and weight and body mass index (r= 0.315, r = 0.221).
Conclusions
The present study was conducted on school going overweight adolescent boys (17-18 years) from district Kurukshetra, Haryana state, India. Meal skipping, more intake of fast foods, carbonated drinks were some of the unhealthy eating habits prevalent among adolescent boys. Therefore, it is necessary to emphasize the importance of regular physical activity and healthy eating habits among adolescents in schools and educate them about adverse effects of fast food so as to prevent future obesity related problems like dyslipidemia, hypertension and diabetes mellitus
References
Anderson JW and Patterson K (2005) Snack Foods: Comparing Nutritional Values of Excellent Choices and Junk Foods. J. Am. Coll. Nutr 24(3): 155-156.
Augustine LF and Poojara RH (2003) Prevalence of Obesity, Weight Perceptions and Weight Control Practices among Urban College Going Girls. Ind. J. of Comm. Medic, 28(4): 187-190.
Australian Bureau of Statistics (1995) National Nutrition Survey: Foods Eaten - Report No. 4804, Canberra, Australia.
Brahmam GNV, Laxmaiah A, Rao KM and Reddy CG (2005) Methodology on Assessment of Diet and Nutritional Status of Community. Pre Conference Workshop on Epidemoiological Tools in Assessment of Nutrition, National Institute of Nutrition, Indian Council of Medical Research: 1-18.
Chhibber C (2010) Children Hooked to Junk Food: Schools Fail to Curb the Menace.The Tribune, Ludhiana, September.
French SA, Story M, Neumark SD, Fulkerson JA and Hannan P (2001) Fast Food Restaurant Use among Adolescents: Associations with Nutrient Intake, Food Choices and Behavioral and Psychosocial Variables. Int J Obes 25: 1823-33.
Galhotra A, Abrol A, Agarwal N, Goel NK and Gupta S (2009) Life Style Related Risk Factors for Cardiovascular Diseases in Indian Ado¬lescents. Internet J Health 9(2).
Gomathy R and John S (2008) Measuring Psychosocial, Environmental and Behavioural Factors that Influence the Fruit and Vegetable Intake of Adolescent Girls. J. Ind. Dietet. Assoc 33(2): 26-37.
Gupta AK and Ahmed AJ (1990) Childhood Obesity and Hypertension. Indian Pediatr 27: 333-337.
Jackson P, Romo MM, Castillo MA and Castillo DC (2004) Junk Food Consumption and Child Nutrition - Nutritional Anthropological Analysis. Rev. Med. Chil 132(10): 1235-42.
Kapil U, Singh P and Pathak P (2002) Prevalence of Obesity among Affluent Adolescent School Children in Delhi. Indian Pediatr 29: 450-452.
Klesges RC, Klesges LM and Shelton ML (1995) A Longitudinal Analysis of Accelerated Weight Gain in Preschool Children. Pediatr, 95: 126-30
Lobstein T, Baur L, Uauy R (2004) Obesity in Children and Young People: A Crisis in Public Health. Obes. Rev 5(Suppl 1): 4 –104.
Lytle LA, Seifert S, Greenstein J and McGovern P (2000) How do Children’s Eating Patterns and Food Choices Change Over Time - Results from a Cohort Study. Am. J. Health Promot 14: 222–228.
Musaiger AO and Gregory WB (1992) Dietary Habits of School-Children in Bahrain. J Royal Soc Health 112: 159-162.
Must A and Strauss RS (1999) Risks and Consequences of Childhood and Adolescent Obesity. Int J Obes, 23(S2): 2-11.
National Institute of Health (1998) Clinical Guidelines on the Identification, Evaluation and Treatment of Overweight and Obesity in Adults. USA: National Institute of Health.
Neumark SD, Story M, Resnick MD, and Blum RW (1996) Corre¬lates of Inadequate Fruit and Vegetable Consumption among Adolescents. Prev Med 25(5): 497-505.
Nielsen SJ, and Popkin BM (2004) Changes in Beverage Intake between 1977 and 2001. Am. J. Prev. Med 27: 205–210.
Niemeier HM, Raynor HA, Lloyd REE, Rogers M.L. and Wing RR (2006): Fast Food Consumption and Breakfast Skipping: Predictors of Weight Gain from Adolescence to Adulthood in a Nationally Representative Sample. J. Adolesc. Health, 39: 842-849.
Singh P and Singh A (2008) Increasing Allurement for Fast Food in Adolescent Girls of Urban Area, Varanasi. Ind. J. Prev. Soc. Med 39 (1and 2): 24-27.
Wolfe WS, Campbell CC, Frongillo EA, Haas JD, and Melink T.A (1994) Overweight School Children in New York State: Prevalence and Characteristics. Am. J. Public Health 84: 807-813.