Alleviation: An International Journal of Nutrition, Gender & Social Development, ISSN 2348-9340
Volume 3, Number 3 (2016) : 1-17
©Arya PG College, Panipat & Business Press India Publication, Delhi
www.aryapgcollege.com, www.apcjournals.com
Assessment of Nutritional Status and Risk of Developing Disordered Eating Among Late Adolescents (18-22 Years) of Chandigarh
Dr. Ritu Pradhan Assistant Professor & Shweta Suri Post Graduate Student
Department of Foods and Nutrition, Government Home Science College, Chandigarh (UT), India
*Email: sharmapritu@yahoo.com
Introduction
The word “Adolescence” is derived from the Latin word ‘adolescere’ which means “the period in a person’s life between childhood and maturity.” Adolescent years are one of the most difficult periods in one’s life time. Urge to come out of the productive umbrella increases and craving to try out new experiences intensify. The last phase in this ladder is “late adolescence phase”, one of the most complex periods in one’s life time (Murat Bas et al 2004).
Due to rapid accretion of tissues and other widespread developmental changes, nutritional needs are more during this period of adolescent’s life cycle. However, the transition from childhood into late adolescence characterizes undesirable changes within the eating attitude of adolescents such as increased consumption of sugar-sweetened beverages (e.g. soda), calorie-dense food, intake of poor snacks, eating food outside the home (e.g. fast foods) and a decline in the intake of milk and other nutrient-rich foods (Fiorito 2006).
Today world is undergoing “Nutrition Transition” which has shown a great impact over the globe. The persistent emphasis of our society on thinness and its characterization of obesity as unacceptable may predispose adolescents, towards irregular eating and induce irregular dietary behaviors further causing disordered eating, that may prove deleterious to adolescent’s health.
In the recent years, some traits have become an important part of youth’s dietary pattern fluctuating their eating behavior and choices of food selection, further characterizing the unfavorable diet of college students. These traits are missing meal, snacking, eating meal away from home and dieting leading to disordered eating behaviors among adolescents. It is commonly accepted that women – particularly adolescent girls – are among its main sufferers. In fact, these disorders seen in an eating pattern have been labeled “maiden disease” (Wilson et al 2005).
The problem of disordered eating can be due to either over indulgence or avoidance of food. Psychological explanation views this disorder as a form of identity crisis, a sign that sufferer blocks emotions, which are expressed through abnormal body image and food intake (Tiemeyer 2008).
Clinical and population studies of women have consistently demonstrated an increased association of anxiety and depression with a risk factor for development of incident disorders in adolescence eating attitude (Patton 1999).
Night Eating Syndrome (NES) is one such disorder where the affected person wakes up several times during the night and is not able to fall back asleep unless he/she eats something. Unhealthy eating behaviors, faulty food habits such as omitting main meal, odd sleeping hours and frequent snacking prevalent among adolescents, also are the causes of night snacking (Brugman et al 1997 & Vatnani 1998).
Keeping the above in mind, the objectives of the present study were:
1) To determine the risk of disordered eating pattern among the subjects using EAT-26.
2) To study the pattern of night eating syndrome among college students.
Methodology
Location of the Study
Five co-educational institutions (Government and private colleges of Chandigarh, department of law of Punjab University) were selected using purposive random sampling method.
Sample Size
All the subjects, day scholars and hostelers, present on the day of survey were included in the study
Data Collection
Self developed, structured, closed ended questionnaire was used for data collection on demographic and dietary pattern. For testing the risk of development of eating disorders, standardized questionnaire “Eating Attitude Test-26” was used.
Eating Attitude Test-26 (EAT-26): EAT-26 (Developed by Paul et al 1979 & Garner et al 1982) was administered to the subjects.
EAT-26 helps to analyze whether the person is symptomatic or asymptomatic for the risk of disordered eating. EAT-26 explores the area related to behavior and attitude regarding food like, preoccupation with food, dietary behavior, concept of body image and its implication of eating and after meal behavior and also self reported binge eating, self induced vomiting and laxative use etc.
This test is also used in many Indian studies by Sridhar (2007) and Solanki (2008) so to access the eating attitude and disordered eating among various groups.
This scale consists of 26 items tapping into eating problems of dieting, bulimia and food preoccupation and oral control. Statements are rated on a 5-point scale ranging from never to rarely, sometimes, often, and usually to always. Answers marked as never, rarely and sometimes carry zero points while often = 1, usually = 2 and always = 3 points, except the last item which is reverse-coded. Respondents scoring ≥ 20 were considered 'at risk' of disordered eating (Garner et al 1982). Hence, summing the scores derives the overall EAT scores.
Standardized techniques were utilized for measurement of anthropometric indices and subjects were classified using BMI classification.
Body Mass Index (BMI): This is a measure of the relative body fatness to evaluate the risk factors associated with obesity.
Pretesting (Pilot Study)
Pre testing was conducted before the actual survey. The questionnaire was pre tested on 10 adolescents in the age group of 18-22 years.
Operational Terms Used in the Study
Late adolescents: Late adolescents represent a unique period of transition between youth and adulthood. It is a last phase of adolescent’s stage and lasts from 18-22 years.
Disordered eating: Disordered eating is a term used to describe irregular eating habits or patterns. A person with disordered eating has a self-directed, faulty pattern of eating that seems beyond the person's control.
Binge eating: It consists of uncontrollable over eating. These types of people consume an excessive amount of food and feel out of control during the binges. People with binge eating disorder also may:
• Eat very quickly than usual during binge episodes.
• Eat till uncomfortably full.
• Eat even when not hungry.
• Because of embarrassment, eat alone.
• Feel guilty, disgusted or depressed after overeating.
Eat-26: The identification of sub-clinical cases of disordered eating was facilitated by the use of this reliable screening procedure (Developed by Paul et al 1979 & Garner et al 1982) to evaluate a broad range of eating attitude and behavior regarding food.
It should be noted that , one of the sentence in the EAT i.e Do you often think of committing suicide was changed to Do you often think of hurting yourself , as it (Suicide) may give negative feedback to the adolescents. So suicidal tendency was changed to hurting themselves.
Snacking: A light, quick meal eaten between, or instead of a main meal. Snacks have a bad reputation, but the wise use of nutritious snacks can improve the health and vitality.
Night eating syndrome: It is a disorder where the affected individual wakes up several times during the night and is not able to fall back asleep unless eats something. When sleeping and eating patterns are simultaneously affected, often there is spectrum of disease that may result and often leads to NES and therefore prolonged stress mostly lead to obsessive disorder i.e. night eating syndrome.
Laxatives: These are taken to induce bowel movements or to loosen the stool, to treat constipation. Sufficiently high doses of laxatives cause diarrhoea.
Diuretic: It is taken to elevate the rate of urination and helps in forced diuresis.
Diet pills: This helps people to curb their hunger and helps to lose weight.
Self induced vomiting: Vomiting produced by administration of ipecac syrup, soapy water, or hand washing liquid detergent or by insertion of a finger or blunt instrument into the throat results in self induced vomiting.
Insomnia: It is concerned with poor sleep that is often broken many times during the course of the night.
Results and Discussion
The present study entitled “Assessment of risk of developing disordered eating among late adolescents (18-22 years) of Chandigarh” was conducted with the objective of assessing the symptoms of disordered eating and night eating pattern of college students.
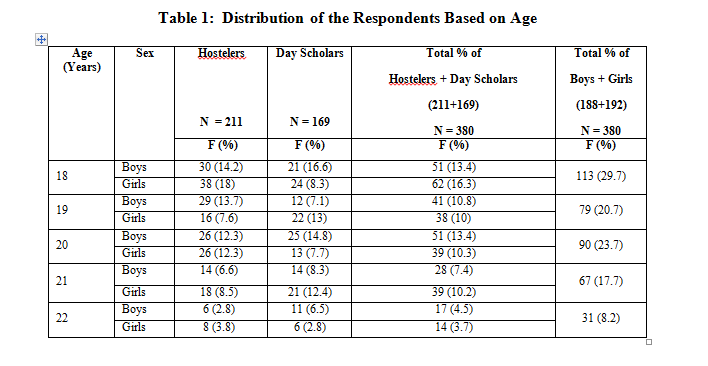
Out of total 380 respondents, total number of boys were 188 while girls were 192, the number of hostelers were 211 and day scholars were 169 (Table 1). Majority of the respondents (29.7%) were of 18 years of age, followed by 20 years of age (23.7%), 19 years of age (20.7%), 21 years of age (17.7%), and 22 years of age (8.2%).
Various studies reported that pocket money also plays an important role in fluctuating the eating pattern of adolescents. Pocket money is the money given to children to take care of petty expenses. This amount of money can be given by parents every day, every week or every month so to fulfill their child needs.
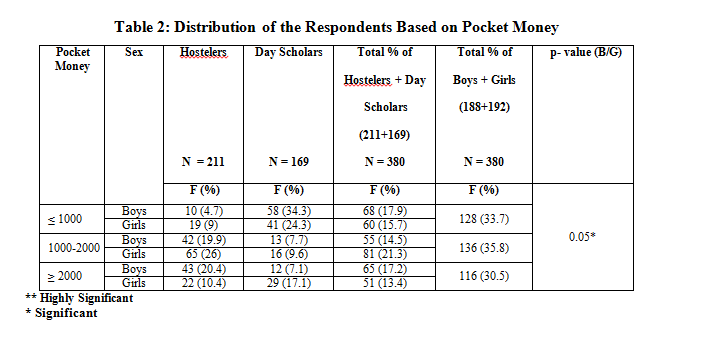
Maximum percentage i.e. 35.8 per cent of respondents’ were given the pocket money around 1000-2000 per month (Table 2). Comparatively a smaller percentage 30.5 per cent received a pocket money of Rs. >2000 per month. It was found that > Rs. 2000 pocket money, was received more by hostelers i.e. 20.4 per cent boys and 10.4 per cent girls than day scholars, chi square value when applied between hosteler and day scholar respondents indicated highly significant difference of (p-value <0.01) with the hostelers getting more pocket money than day scholars while 35.8 per cent of respondents were given the money up to Rs.1000-2000 per month, out of which percentage of girls was quite more than the boys and the difference between boys’ and girls’ pocket money was significant (p-value <0.05), due to the fact that girls spend more being more concerned about their looks and self.
The study thus indicates that higher number of girls and hostelers group get more pocket money irrespective of their needs and requirements.
Hence pocket money given to adolescents renders a sense of independence and responsibility towards spending the money the right way and gets them into the habit of planning income and expenditure. They also learn about saving and budgeting.
Thus it clearly indicates that hostel respondents indulge in higher level of spending on food items than day scholars. The highest percentage of money is spent on food items due to the fact that, now a days ‘pigging out’ have become a common practice by college students. Just to have fun with foods while socializing with friends have rendered the scenario and this only has led them to spend more and more money on food items. Ready-to-eat and fast food are usually eaten along with friends. Gradually this becomes a habit, resulting in a host of malnutrition related problems.
So it is clear that adolescents’ eating habits can endanger health, as many adolescents receive inadequate nutrition due to poor diets, moreover irregular eating habits and eating disorders also stems into society's idealization because the preference given to thinness and other faulty aspects which further results not only in health complications but irregular and disturbed sleep pattern within them.
Adequate and sound sleep is also one of the critical factors of health and health-related behavior in adolescents and sound sleep influences physical and emotional well-being (Redeker 2004).
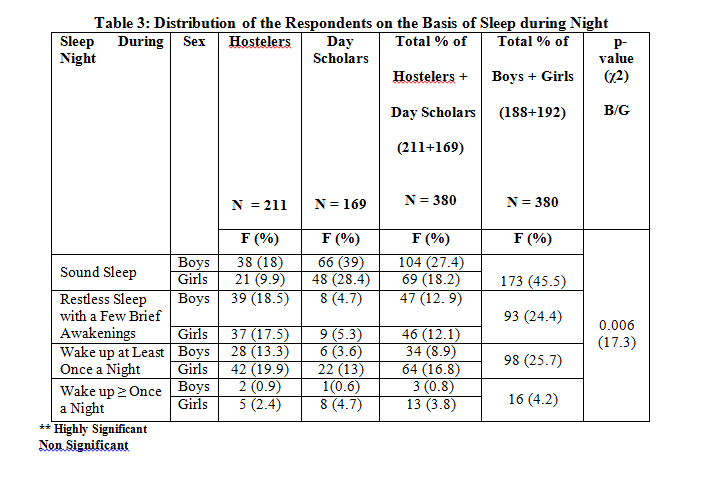
Only 45.5 per cent of respondents enjoyed sound sleep, out of which percentage of day scholar boys was more, while 25.7 per cent of respondents used to wake up at least once a night, followed by restless sleeps with a few brief awakenings (24.4 %) and waking up more than once a night (4.2%) (Table 3). Inadequate sleep was more seen among hostelers showing more significant results (p-value <0.01) than day scholars with the reason that hostlers are late sleepers and they often snack at night and more over no one is there to object their habits, but chi square value when applied between boys and girls did not show any significant difference.
Looking at the sleep scenario among adolescents, pattern has been disturbed not only because of the work load but also due to the life style changes and snacking at night is one example of this.
It can be seen from Table 4 that 52.3 per cent of respondents were in the habit of snacking after dinner while 47.7 per cent denied the habit of night snacking. Among 52.3 per cent of respondents who snacked at night, hostelers were more than day scholars.
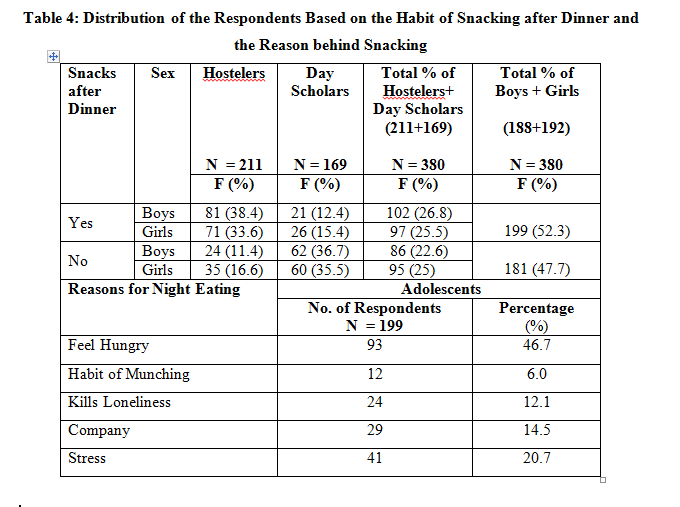
The main reason recorded from the respondents, was being hungry what persuades them to snack at night time which was approved by 46.7 per cent of respondents while 20.7 per cent said that out of stress, they snack, as eating at such time helped them to divert their attention and 14.5 per cent and 12.1 per cent respondents reported that night eating was done more in company and group gathering and moreover it also killed loneliness while only 6.0 per cent respondents did night eating out of their habit of munching.
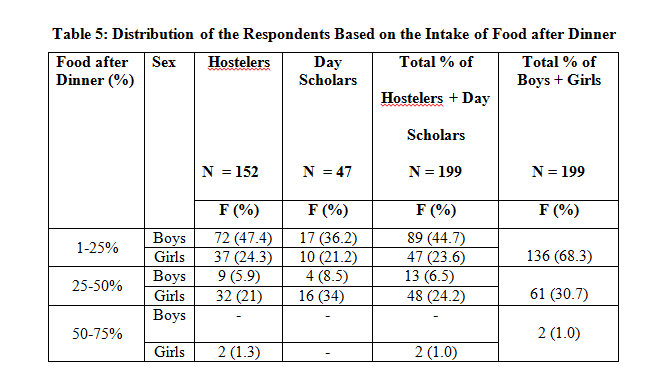
Night Eating Syndrome (NES) is characterized by a lack of appetite in the morning, consumption of more than 25-50 per cent or more of daily food intake after dinner. Out of total 380 respondents, only 52.3 per cent used to eat at night. Out of those who snacked at night, 1-25 per cent intake of snacks after dinner was seen among 68.3 per cent of respondents while 30.7 per cent followed 25-50 per cent intake of food after dinner and 1 per cent ate more than 50 per cent after dinner meeting up the criteria of night eating syndrome (Table 5).
The results depicted that hostlers were highly involved in eating snacks after dinner than day- scholars due to the reason that, hostelers have more fluctuating eating pattern as there is no one to take care of them, moreover late night sleeping and getting up late habit is also one of the reason behind late night snacking among hostelers rather than day- scholars.
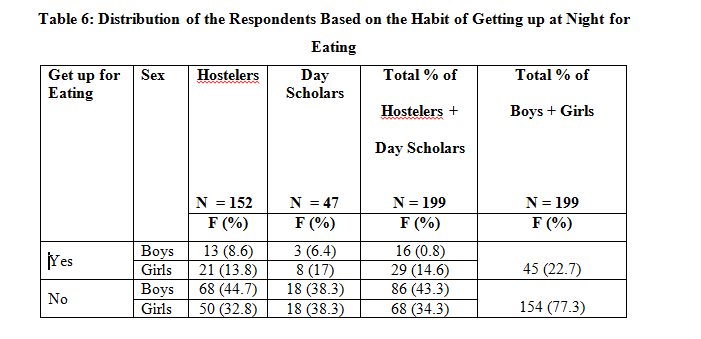
It is visible from the Table 6 that only 22.7 per cent had a habit of getting up in the middle of the night for eating, out of which the number of hosteler girls were more than hostler boys
It can be seen from the Table 7 that 40.2 per cent of respondents were undergoing night eating problem since months while 34.1 per cent respondents since years. The maximum percentage was seen among hostelers who had been undergoing this habit since months and years, due to the fact that once habit is developed, it is difficult to get out of it and moreover, hostlers often tend to eat more as no one is there to keep a watch on their eating behavior which further demolishes their eating behavior, thus making them eat at any time and eating whenever and whatever they want.
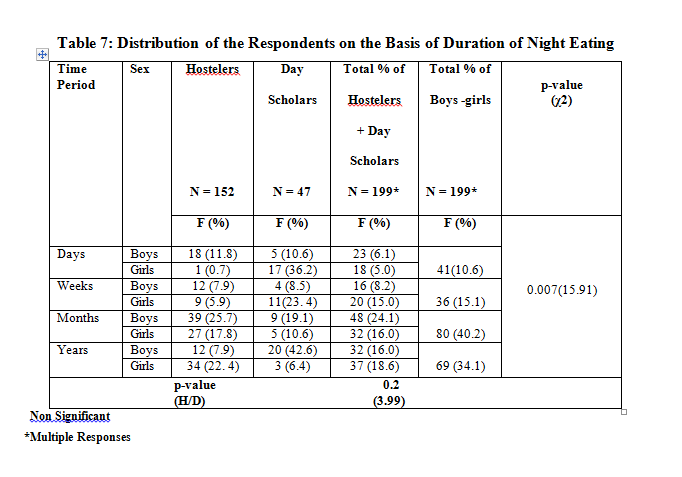
This only prompts hostlers group to eat large quantities of food during the evening hours usually after depriving themselves of food during the day. Sometimes, being unconscious of this behavior and unaware of how many calories they’re consuming, adolescents suffer from night snacking syndrome.
Stress can have a big effect on a person's eating habits and can lead to psychological problems. A positive correlation (0.298**) was found between the adolescents suffering from stress and night snacking (p-value <0.01). Results depicted that almost half the percentage of total adolescents who snacked at night suffered from stress, which was found among 40.0 per cent studied respondents, thus it could be concluded that stress is directly related to night eating syndrome. Grilo et al (2005) in one of his study concluded that stress and depressive symptoms were greater found in the NES people and these participants ate fewer meals during the day and more during the night to cope up with their stress.
Thus, conditions are exaggerated and may result in causing a disordered eating and further causing eating disorders among adolescents. Keeping this criteria in mind, an attempt was made to know whether the adolescents were symptomatic of disordered eating symptoms, EAT-26 was considered for this, it is a screening test to identify sub-clinical cases of disordered eating made by Garner et al (1982).
EAT-26 is an efficient screening instrument as part of a two-stage screening process in which those who score at or above a cut-off score of 20 are referred for being a symptomatic for disordered eating. EAT-26 explores the area related to behavior and attitude regarding food like, Preoccupation with food, dietary behavior, concept of body image and its implication of eating and after meal behavior and also self reported binge eating, self induced vomiting and laxative use etc. This test is also used in many Indian studies by Sridhar (2007) and Solanki (2008) so to access the eating attitude and disordered eating among various groups.
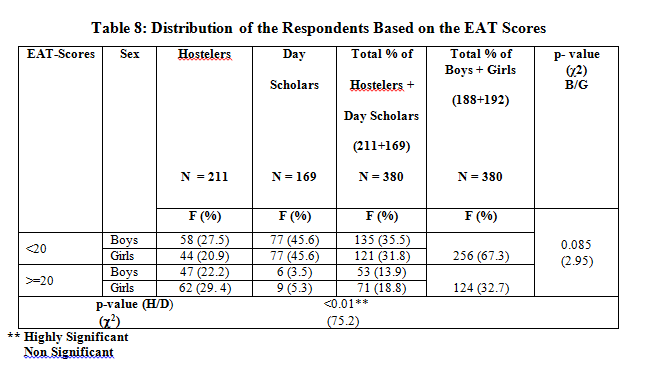
It is indicated in Table 8 that 32.7 per cent of respondents were symptomatic of disordered eating, as they scored >=20 in the EAT, chi square value when applied between total boys and girls having EAT scores above 20 for disordered eating did not reveal significant difference while a high significant difference (p-value <0.01) was found among hostelers and day scholars group where maximum responses were seen among girls hostelers i.e. 29.4 per cent who came out to be more symptomatic as they were more preoccupied with the desire to be thinner, ate diet food, undergo binges etc. High scores on Eating Attitude Test revealed that there was the percentage of adolescents who proved to be symptomatic, putting a great question on their eating pattern and life style.
Studies by Solanki (2008) suggested that several characteristics of dietary behavior such as eating frequency, the temporal distribution of eating events across the day, breakfast skipping, and the frequency of meals eaten away from home, odd time snacking together referred to as "eating patterns," when such eating patterns get altered often result in high score on Eating Attitude Test, thus causing a disordered eating among person.
Disordered eating also consists of episodes of uncontrollable overeating or troublesome eating behaviors, such as restrictive dieting, bingeing, or purging in which people consume huge amounts of food while feeling out of control and powerless to stop such as bingeing on food.
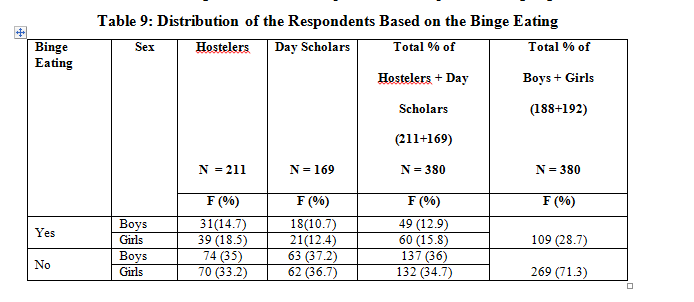
Furthermore, it can be seen from Fig 9 that 28.7 per cent of respondents were engaged in binge eating, followed more by girls and more among hostlers in comparison to their counter parts. The fact that out of taste and while sitting in one’s company, one tends to eat more, furthermore dieting and fasting also often contribute to binge eating among girls, leading to uncontrolled eating behaviors. Adolescents also eat more when stressed and this is quite likely to become a routine altering the eating attitude.
The Table 10 indicates that 4.4 per cent of respondents engaged themselves in self induced vomiting, out of which percentage of girls was little more, as girls are more conscious about their looks so in order to get rid off excess food calories, this type of behavior is mostly shown by them.
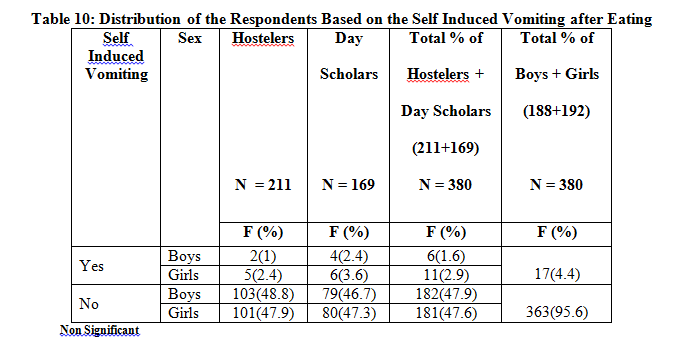
Adolescents afraid to stop such kind of destructive practices because of out of control eating and without the use of vomiting, they often fear, they will become grossly overweight and due to this reason, adolescents switch themselves towards other psychological disorders like intake of laxatives, diet pills etc which also lead them towards depression and anxiety.
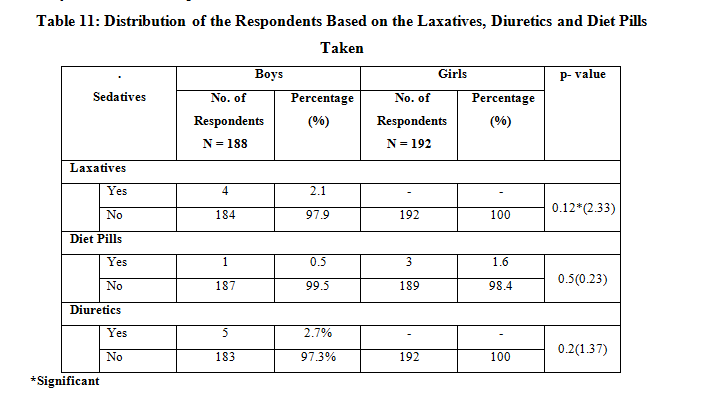
It is clear from the Table 11 that 2.1 per cent of boys used laxatives (Products that promote bowel movements and helps in weight loss) that was significant (p-value <0.05) in comparison to girls when chi square test was applied while 2.7 per cent of boys were engaged in diuretics (Drugs that tends to increase the discharge of urine) and diet pills (Capsule containing chemical substances that aid in controlling body weight by suppressing the appetite) were taken by 0.5 per cent boys and 1.6 per cent girls respectively that came out to be non significant.
The data clearly mentioned that in order to lose weight, adolescents mostly switched over to faulty methods like diet pills, laxatives, diuretics etc.
An attempt was made to know whether respondents hurt themselves, it can be seen in the Table 12 that 5.8 per cent of respondents committed such behaviors, out of which the percentage of boys (3.7 %) was quite more than the girls (2.1%)
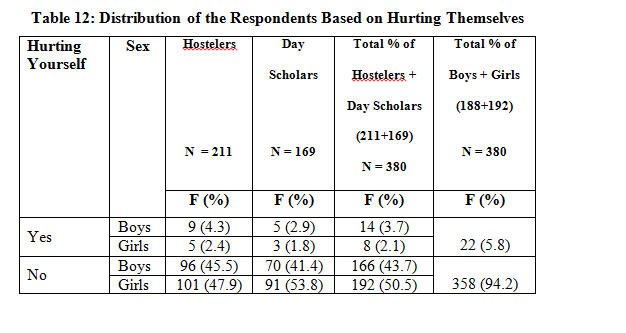
Self hurting is undertaken by adolescents because of disordered eating as; these disorders encompass a wide variety of behavioral problems, ranging from pervasive developmental disorders which may severely affect many aspects of psychological development, thus causing abnormal, behavioral problems like hurting themselves as shown by most adolescents.
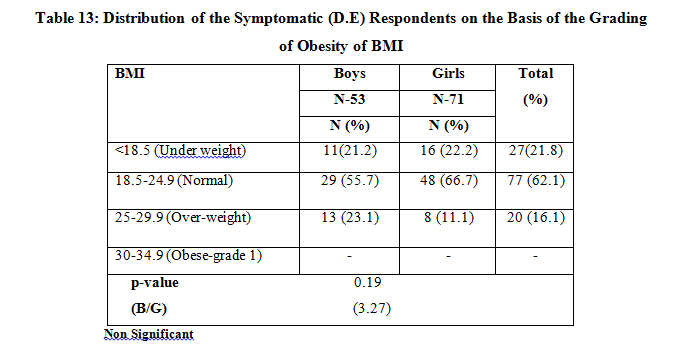
BMI is commonly used as a measure of adiposity. The Table 13 depicts those respondents who came out to be the symptomatic for disordered eating and when analyzed revealed that majority of (55.7%) respondents from boys group and 66.7 per cent from girls group were normal. Almost a similar number i.e. 21.2 per cent of boys and 22.2 per cent girls were underweight. The more prevalence of underweight was seen among girls, as compared to boys which may be due to the girls’ low nutrient intake and undergoing dieting, also 11.1 per cent of girls and 23.1 per cent of boys were overweight. This prevalence of overweight and obesity in the respondents is probably due to high fat intake and snacking habits in between meal. Girls were underweight as compared to boys. A significant difference was found in the BMI of boys and girls.
Conclusions
The changes in the eating attitude and diet pattern, over consciousness about self regarding looks, over concerned about weight gain and loss, increase in the pocket money, trend of increased eating out frequency, odd time snacking habit have been found to be the inherent part of the life of young students which have lead to the disordered eating behavior among adolescents.
The present study too, found that poor food habits, irregular meal timings, unhealthy snacking and skipping of meals were more prevalent among the respondents. Majority of the respondents snacked at night, not only to curb their appetite but also to kill their loneliness. Fast foods, junk and fried food items were being the most liked by the adolescents, as maximum respondents spend almost half of their pocket money on such unhealthy foods while healthy food stuffs like milk and fruits were almost given no preference.
Therefore, to conclude it can be said that increased energy intake with decrease in the physical activity, increased eating out frequency and nibbling have led to significant changes in the eating pattern and life style of late adolescents. These fluctuating and changed dietary patterns together could force the youngsters at risk of various chronic illnesses, further causing clinical eating disorders. So awareness regarding healthy eating with increased physical activity and control over eating behavior is needed to secure the health of youth. As adolescents are the future generation, who will be further associating their own families and further be responsible for bringing in healthy balanced meals to their family members and inculcating healthy food habits in their children, therefore, there is a need of bringing awareness about the higher prevalence of abnormal eating patterns and attitude among the adolescents.
References
Brugman E, Meulmeester JF, Spee-van der Wekke A, Beuker RJ, Zaadstra BM, Radder JJ Fiorito LM, Mitchell DC, Smiciklas WH, and Birch LL (2006) Dairy and Dairy- Related Nutrient Intake during Middle Childhood. J Am Diet Assoc 106:534–542.
Garner MD, Olmsted MP, Bohr Y, and Garfinkel PE (1982) The Eating Attitudes Test: Psychometric Features and Clinical Correlates. Psychological Medicine 112: 871-878.
Grilo CM, Carlos M, Allison KC, Masheb RM, and Stunkard A (2005) Binge Eating Disorder and Night Eating Syndrome: A Comparative Study of Disordered Eating, Journal of Consulting and Clinical Psychology, 73 (6): 1107-15.
Murat BF, Hulya A, Efsun K, and Gul K (2004) Eating Attitudes and Their Psychological Correlates among Turkish Adolescents. Adolescence 39 (1): 8-53.
Neumark SD and Hannan PJ (2009) Weight-Related Behaviors among Adolescent Girls and Boys. Arch Pediatr Adolesc Med 154: 569–577.
Patton GC, Johnson SE, Wood K, Mann AH, and Wakeling A (1999) Abnormal Eating Attitudes in London Schoolgirls—A Prospective Epidemiological Study: Outcome at Twelve-Month Follow-up. Psychol Med 20: 383–394.
Paul EG, Garner DM, and Garfinkel PE (1979) The EAT: An Index of The Symptoms of Anorexia Nervosa. Journal of Psychology and Medicine 9: 273-279.
Redeker NS, Rugiero JS, and Hedges C (2004) Sleep is Related to Physical Function and Emotional Well-Being after Cardiac Surgery. Nurs Res 53: 154-162.
Solanki RK, Paliwal A, Singh P, Swami MK and Midha A (2008) Psychiatric Correlates of Obesity in Women and its Impact on Quality of Life. Indian Journal of Psychology 30 (1):52-58.
Sridhar GR (2007) Psychiatric Co-Morbidity and Diabetes. Indian J Med Res 125: 311-320.
Tieyer MJ (2008) Disordered Eating Across the Life Span. Am J Diet Assoc 104: 1208. –1210.
Vatnani G (1998) Nutrition Profile of Obese Vs Non- obese Affluent Adolescent Girls (16–18Years), M Sc Dissertation, University of Delhi, Delhi.
Wilson GRS (2005) Eating Disorders Guidelines from NICE. J of Medicine & Science in Sports & Exercise 365 (9453): 79-81.