Alleviation: An International Journal of Nutrition, Gender & Social Development, ISSN 2348-9340
Volume 7, Number 7 (2020): 1-11
© Arya PG College (College with Potential for Excellence Status by UGC) & Business Press India Publication, Delhi
http://apcjournals.com, www.aryapgcollege.com
An Appraisal of the Nutritional Status of Children of the Age Group of 5-10 Years Suffering from Cerebral Palsy
Anjali Dewan
Associate Professor and Head (Retd.), Department of Home Science
St. Bede’s College, Shimla
(Himachal Pradesh), India
Email: dewananjali2014@gmail.com
Abstract
The term cerebral palsy is used to any one of a number of neurological disorders that appear in infancy or early childhood and permanently affect body movements and muscle coordination but are not progressive. It results in less cognitive development, poor learning ability, low IQ, impaired growth and development. The children suffering from this disorder are unable to feed themselves due to impairment in their feeding skills. This generally results in malnutrition due to diminished food intake. The present study was carried out on 100 children in the age group of 5-10 years from two schools for disabled children in Shimla. A pre-tested questionnaire was used to collect data by interviewing mothers of the children suffering from cerebral palsy to know about their dietary pattern and problems faced during feeding them. Anthropometric measurements, clinical signs of various deficiencies observed in children were noted down. The results showed that there was a significant relationship between oral-motor dysfunction and their nutritional status. If there is early detection of this disorder, there will be less deteriorative effects on the physical growth and health of these children. There is no cure for cerebral palsy, but supportive treatments, medications and surgery can help many individuals improve their motor skills and ability to communicate with the world.
Keywords: Anthropometry, Cerebral Palsy, Dysfunction, Feeding, Nutrition, Nutritional Status.
Introduction
The term cerebral palsy is used to any one of a number of neurological disorders that appear in infancy or early childhood and permanently affect body movements and muscle coordination but are not progressive, in other words, they don’t get worse over time. The term cerebral refers to the two halves or hemispheres of the brain, in this case to the motor area of the brain’s outer layer (cerebral cortex), the part of the brain that directs muscle movements, palsy refers to the loss or impairment of motor function. Even though cerebral palsy affects muscle movement, it is not caused by problems in the muscles or nerves (Stanton 1992). It is caused by abnormalities inside the brain that disrupt the brain’s ability to control movements and posture. In some cases of cerebral palsy, the cerebral motor cortex has not developed normally during foetal growth (Geralis 1991). In other words, the damage is a result of injury to the brain either before, during, or after birth. In either case, the damage is not repairable and the disabilities that result are permanent. Children with cerebral palsy exhibit a wide variety of symptoms e.g.
• Lack of muscle coordination when performing voluntary movements (ataxia).
• Stiff or tight muscles and exaggerated reflexes (spasticity).
• Walking with one foot or leg dragging.
• Walking on the toes, a crouched gait or a scissored gait.
• Variations in muscle tone, either too stiff or too floppy.
• Excessive drooling or difficulties swallowing or speaking.
• Shaking (tremor) or random involuntary movements.
• Difficulty with precise motions, such as writing or buttoning a shirt.
The symptoms of cerebral palsy differ in type and severity from one person to the next, and may even change in an individual over time. Some people with cerebral palsy also have other medical disorders including mental retardation, seizures, impaired vision or hearing and abnormal physical sensations or perceptions. Cerebral palsy does not always cause profound disabilities. While one child with severe cerebral palsy might be unable to walk and need extensive, lifelong care (Cogher & Smith MF 1992) another with mild cerebral palsy might be only slightly awkward and require no special assistance (Paul 2000).
A syndrome called failure to thrive is common in children with moderate-to-severe cerebral palsy. In babies, this lag usually takes the form of too little weight gain (Griffths & Clegg 1988). In young children, it can appear as abnormal shortness and in teenagers, it may appear as a combination of shortness and lack of sexual development. In addition, the muscles and limbs affected by cerebral palsy tend to be smaller than normal (Cogher & Smith MF 1992) . Children with cerebral palsy have difficulty eating and drinking because they have little control over the muscles that move their mouth, jaws and tongue. They are also at risk for breathing food or fluid into the lungs. Some children develop gastroesophageal reflux disease (GERD commonly called heartburn) in which a weak diaphragm cannot keep stomach acids from spilling into the oesophagus. The irritation of the acid can cause bleeding and pain. They are also at risk for malnutrition, recurrent lung infections and progressive lung disease (Zinkin and McConachie 1995).
The present study was planned to assess the nutritional status of selected children afflicted with cerebral palsy attending two schools especially for disabled children. This was accomplished with the help of anthropometric measurements, clinical signs of nutritional deficiencies and dietary evaluation.
Materials and Methods
number of 100 children suffering from cerebral palsy were selected from two schools of disabled children in Shimla. The place selected for conducting the present study was Shimla.
Hundred children suffering from cerebral palsy were selected from two schools for disabled children in Shimla.
Purposive sampling was used to select the respondents. In some cases, the mothers of the respondents had to be convinced to actively participate in the research work. A meeting was arranged with the mothers of the selected respondents to confirm their participation in the study. The subjects selected for this study were all children and belonged to different income groups. The age of the subjects ranged between 5-10 years. The data were collected from May 2018 to October 2019.
The study was conducted on 100 children afflicted with cerebral palsy consisting of 60 boys and 40 girls. A pre-tested questionnaire was filled by the mothers of the children to obtain information regarding age, sex, monthly income, birth order & birth weight etc. The mothers also provided data regarding the introduction of weaning foods, nature of feeding problems and the foods eaten by their children after a three day dietary recall. The children were divided into two broad age groups consisting of 5-8 years, >8-10 years. Anthropometric measurements included weight, height, head, arm and chest circumference, bicristal diameter consisting of the hip width (Wyngarden 1992).
Since the children were unable to stand erect, the height and weight was noted down using indirect methods (Gangopadhyay & Mukherjee 2003). For taking the height, the children were made to lie straight and marks were made touching their head and feet. The distance between these two marks was noted down which denoted the height. In order to weigh the child, the mother was asked to stand on the weighing scale with her child and then she was asked to stand alone on the weighing scale. The difference between the two readings was the exact weight of the child. Clinical examination of the children was done using ICMR clinical assessment form.
Results and Discussion
The analysis of the data collected showed that cerebral palsy was found in all the income groups and affects both poor and rich alike (Geralis 1991). When birth order of these children was looked into, it was seen that more than 70 per cent children were first born of their mothers and one third were second in their birth order. It also illustrated that almost 40 per cent children had low birth weight of less than 2 Kg and had a small size at the time of birth.
To obtain the information regarding the oral-motor defect, the pattern of breast feeding revealed that 25 per cent of the children could not be breast fed at all. Continuation of breast feeding till 3 years was common (36.7%). Due to poor oral and motor co-ordination, solid foods were started late in most of the children. The results showed that almost 80 per cent started eating solids at the age of two years and above. About 19 per cent showed difficulty in swallowing food and 25.3 per cent found it difficult to chew the food properly. However, 81 per cent were given foods of normal texture to help in the development of their motor skills.
Anthropometric Measurements of the Respondents
It has been observed that the anthropometric measurements reflect many morphological variations from the normal due to any significant functional physiological change. The results of the various anthropometric measurements (Sankhala et.al. 2004) in comparison with the standard ICMR measurements of the children suffering from cerebral palsy are shown in Table 1, Figure 1 and Table 2, Figure 2.
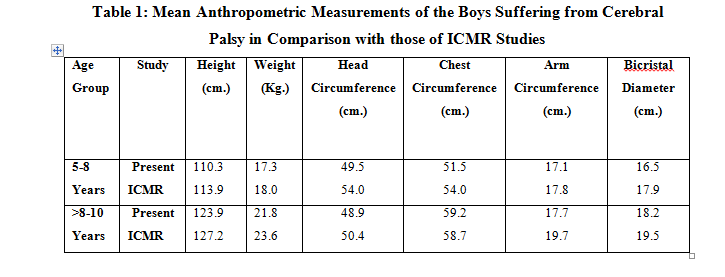
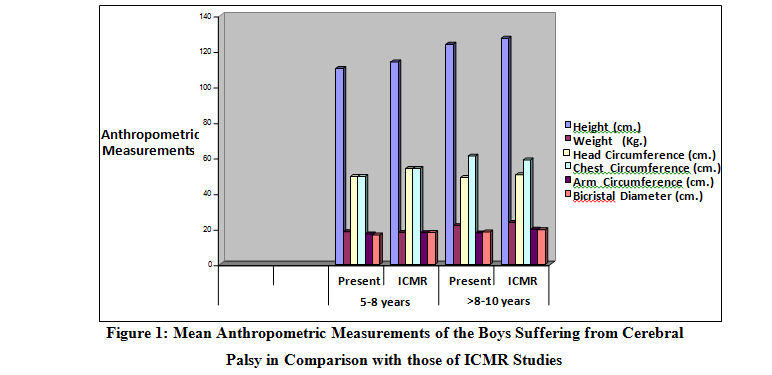
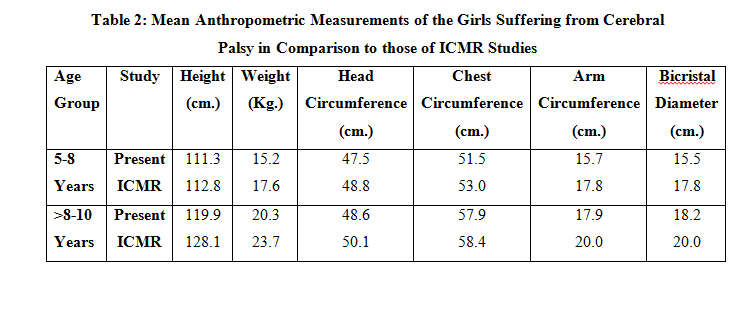
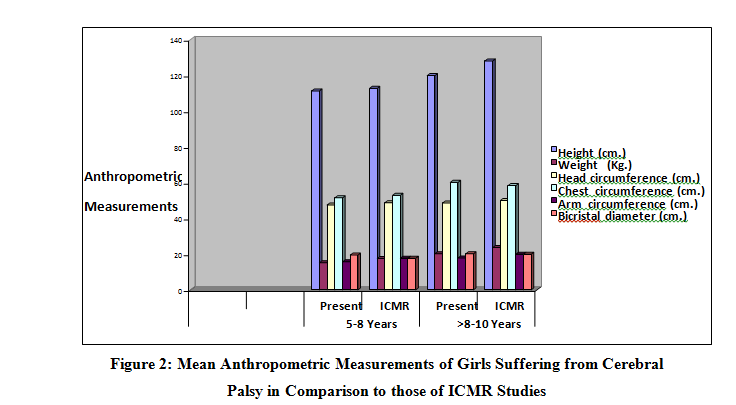
The results showed that there was a a reduction in the height among all groups of boys and girls. A reduction in the height of children according to their age in comparison with ICMR values indicated that either the children were not fed properly or there was a past history of malnutrition. Weight according to age showed a clearer picture about their nutritional status (Pereschel et. al.1995) . The data collected showed that it was less in all the age groups of boys and girls. Head circumference which is primarily related to the size of the brain and thickness of the soft scalp tissues can change with the nutritional status so that it can get affected due to protein calorie malnutrition. From the present study, it was clear that all the above parameters had reduced in almost all the age groups in either sex.
The arm circumference is a good indicator of muscle development. The present study showed a marked reduction as compared to the ICMR studies indicating muscle wasting irrespective of age and sex. Chest circumference did not show much deviation from the normal values. This was not due to optimum nutritional status of the children but due to deformities in the chest area which masked their true chest circumference. Hip width of bicristal diameter though an uncommon index of nutritional status was used as an indicator to show that the hip width of the children was less as compared to the standard value given by ICMR (Indian Council of Medical Research 1990).
Clinical Assessment
Clinical assessment of the children showed that 33.5 per cent of the children were seen as thin built with or without other signs of malnutrition. The clinical signs (Jellife 1966) indicative of the nutritional deficiencies are shown in Table 3.
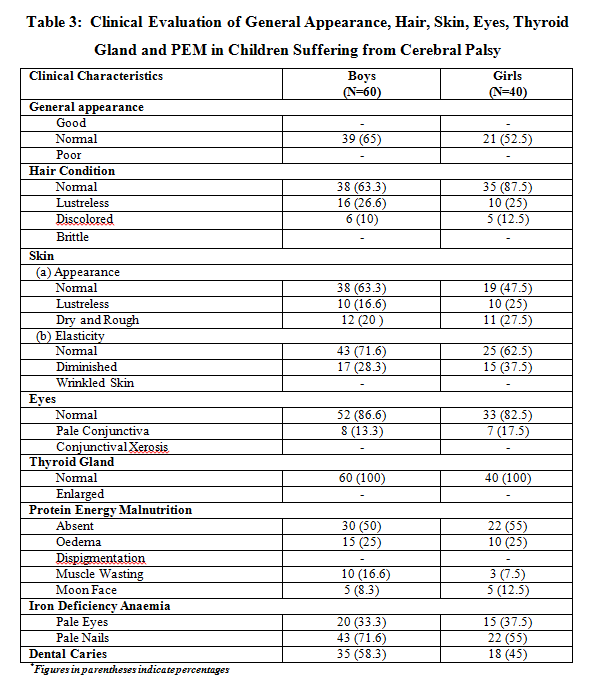
Pale eyes and pale nails were indicative of iron deficiency anaemia was pointed out in some of the children while about 20 per cent had lustreless skin suggesting Vitamin A, C or B complex deficiency. Dental caries affected almost 53 per cent due to the children’s tongue being less mobile and impairment in the cheek bones of many children resulting in teeth not getting properly cleaned. The present study clearly showed that there was a clear and a definite relationship between the feeding problems associated with oral-motor dysfunction in children with cerebral palsy and their growth and nutritional status. In severe cases where swallowing problems are causing malnutrition, a doctor may recommend tube feeding, in which a tube delivers food and nutrients down the throat and into the stomach, or gastrostomy, in which a surgical opening allows a tube to be placed directly into the stomach (Winstok 1994).
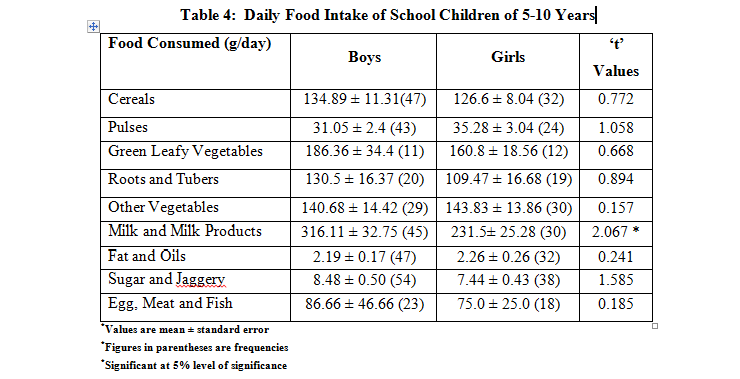
The daily mean consumption of green leafy vegetables by children, both boys and girls, was 186.36 ± 34.4 g and 160.80 ± 18.56 g respectively. The children of both the groups liked spinach, mustard leaves and cabbage the most. The intake from both the categories was adequate and was exceeded as compare to RDI (100g). The average everyday consumption of roots and tubers by boys and girls was 130.50 ± 16.37 g and 109.47 ± 16.88 g respectively. Children of both the groups consumed potato as the main vegetable. Intake of roots and tubers was higher in boys than the girls but the difference was not significant. The daily mean intake of other vegetables by boys and girls was 140.68 g ± 14.42 and 143.83 ± 13.86 g respectively. Intake of other vegetables by boys was slightly less than the girls. This may be because boys disliked most of the vegetables.
The average daily consumption of milk and milk products by boys and girls was 316.11 ± 32.75 g and 231.50 ± 25.28 g respectively. Cow’s milk was generally preferred by children of both the groups as compared to buffalo’s and goat’s milk. The intake was significantly higher than the RDI (500 ml). The overall daily intake of fats and oils by boys and girls respondents was 2.19 ± 0.17 g and 2.26 ± g of the RDI (25 g) respectively. Majority of children took mustard and refined oil. The intake was significantly lower than the RDI by both the groups. Daily mean intake of sugar and jaggery by boys and girls was 8.48 ± 0.50 g 7.44 ± 0.43 g, though the RDI for sugar was 30 g. The intake of sugar and jaggery was significantly lower in both the groups when compared with suggested intakes by ICMR (Indian Council of Medical Research 1990).
Nutrient Intake
Data on the nutrient intake of boys and girl children is summarized in Table 4. The mean consumption of nutrients by children as per cent meets the requirement of ICMR’s RDA (Recommended Dietary Allowance) of nutrients.
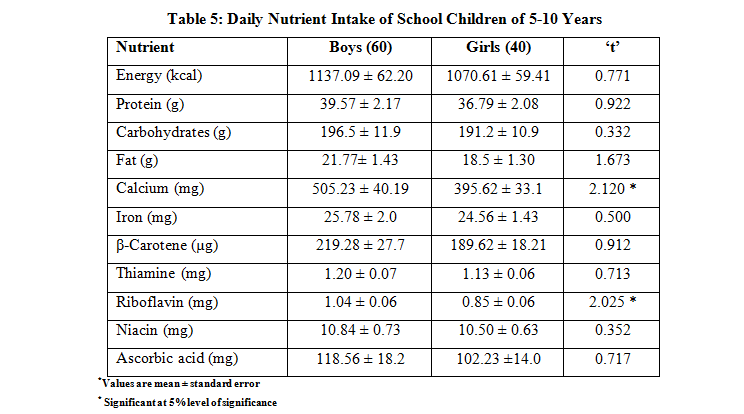
The average daily energy intake by male and female children was 1137.09 ± 62.20 kcal and 1070.61 ± 59.41 kcal respectively meeting 58 per cent and 55 per cent of the RDA. The intake of energy was significantly lower than the RDA (1950 Kcal) in both the groups. The diets were identical in both the schools with no significant difference. The daily mean intake of protein by male children was 39.57 ± 2.17 g which was 96 per cent of the Recommended Dietary Allowances, whereas, the protein intake by female children was 36.79 ± 2.08 g which was 89 per cent of the RDA.
The intake of protein was significantly lower than the RDA (41g) in both the groups. The daily mean intake of fat by male child was 21.77 ± 1.43 g i.e. 87 per cent of RDA whereas intake of fat by female was 18.50 ± 1.30 g, which was 74 per cent of the RDA (25 g). Similar result was reported by (Sankhala et.al 2004). The mean intake of calcium by boys and girls was 505.23 ± 40.19 mg and 395.62 ± 33.16 mg, respectively as compared to the RDA (400 mg) 126 and 98 per cent respectively. It was reported that at base line, calcium intake was inadequate (83% of RDA) (Chawla & Sharma 2007) in both the control and experimental groups which significantly increased to 459 mg in groups after counseling and exceeded the RDA.
Average daily intake of iron by boys and girls was 25.78 ± 2.0 mg and 24.56 ± 1.43 mg respectively which was about 99 per cent and 94 per cent of the RDA (26 mg) respectively. Daily mean intake of β-carotene by male and female children was 219.28 ± 27.7 µg and 189.62 ± 18.21 µg which was 9 per cent and 7.9 per cent. The intake of β-carotene was significantly lower than the RDA (2400 µg). Daily mean consumption of thiamine by male and female school children was 1.20 ± 0.07 mg and 1.13 ± 0.06 mg which was 120 per cent and 113 per cent of the RDA (1.0 mg) respectively. Mean intake of riboflavin by boys was 1.04 ± 0.06 mg which was 86 per cent of the RDA. The intake of riboflavin by girls was 0.85 ± 0.06 mg which was 70 per cent of the RDA (1.2 mg). Mean consumption of niacin by boys was 10.84 ± 0.73 mg, which was 83 per cent of RDA. The intake of niacin by girls was 10.50 ± 0.63 mg, which was 80 per cent. The intake of niacin was less than the RDA (13 mg). It has been reported by other researchers also that the intake of niacin is below the RDA in the diet of children.1 The daily mean intake of ascorbic acid by male and female was 118.56 ± 8.2 mg and 102.23 ± 14.0 mg respectively i.e. more than 100 per cent of the RDA (40 mg).
Cerebral palsy is not a disease. It is not contagious and it cannot be passed from one generation to the next. There is no cure for cerebral palsy, but supportive treatments, medications and surgery can help many individuals improve their motor skills and ability to communicate with the world (Peacock 2000). There is no cure for cerebral palsy, but supportive treatments, medications and surgery can help many individuals improve their motor skills and ability to communicate with the world. Parents of a child newly diagnosed with cerebral palsy are not likely to have the necessary expertise to coordinate the full range of care their child will need (Paul 2000). Although knowledgeable and caring medical professionals are indispensable for developing a care plan, a potentially more important source of information and advice is parents who have dealt with the same set of difficulties.
References
Chawla P and Sharma S (2007) Nutritional Status and Mental Ability of School Girls (7-9 Years) as Influenced by Nutrition Counselling. J. Hum. Ecol. 22 (1): 1-5.
Cogher L, Savage F and Smith MF (1992) Cerebral Palsy-The Child and Young Person. London: Chapman and Hall Medical.
Gangopadhyay D and Mukherjee H (2003) Nutritional Status of Cerebral Palsied Children (3-12 Years). Applied Nutrition 28 (1&2): 28-32.
Geralis E (1991) Children with Cerebral Palsy-A Parent Guide. United States: Woodbine House.
Griffths M and Clegg M (1988) Cerebral Palsy-Problems and Practice. UK: Souvenir Press (Educational and Academic) Ltd.
Indian Council of Medical Research (1990) Nutrient Requirement and Recommended Dietary Allowances for Indians. Hyderabad: National Institute on Nutrition.
Jellife DB (1966) The Assessment of Nutritional Status of Community. Geneva: World Health Organization: 74.
Paul P (2000) Living with Cerebral Palsy. USA: TX: Raintree Steck-Vaughn Publishers.
Peacock J (2000) Cerebral Palsy. Mankato: Capstone Press.
Pereschel SM, Scola PS, Weidenman LE and Bernzer JC (1995) The Special Child. United States: Paul H. Brookes Publishing Company: 163-164.
Sankhala, Aarti, Sankhla AK, Bhatnagar B and Singh A (2004) Dietary Status of Children of Udaipur. Anthropologist 6 (4): 257-259.
Stanton M (1992) Cerebral Palsy-A Practical Guide. United States: Optima, a Division of Little Brown Publishers Ltd.
Winstok A (1994) The Practical Management of Eating and Drinking Difficulties in Children. Winslow: Winslow Press Limited.
Wyngarden BJ (1992) Textbook of Medicine. Philadelphia: W.B. Saunders Company.
Zinkin P and McConachie H (1995) Disabled Children and Developing Countries. London: Mac Keith Press.